Supraglottic Swallow:
In order to perform this swallow the patient must be alert, relatively relaxed, and able to follow simple directions without becoming upset or confused. The patient places food in his mouth while these directions are being given: "Take a deep breath and hold your breath (if the vocal folds are not closed then try different directions like inhale and then say ah, turn off your voice and hold your breath). Keep holding your breath while you swallow. Immediately after you swallow, cough." The patient should practice with saliva prior to food (Logemann, 1998).
Super-Supraglottic Swallow:
This strategy is used in patients with reduced closure of the airway entrance. The effort involved in the super-supraglottic swallow increases the anterior tilt of the arytenoid and the false vocal cord closure to close the entrance to the airway early, before and during the swallow. The patient is given the instructions to "Inhale and hold your breath very tightly, bearing down. Keep holding your breath and bearing down as you swallow. Cough when you are finished (Logemann, 1998)."
Logemann, J. A. (1998). Evaluation and treatment of swallowing disorders (2nd ed.). Austin, TX: Pro-Ed.
.
http://www.ucs.louisiana.edu/~ncr3025/roussel/codi531/COPD2.html
Boden, K., Hallgren A., & Witt Hedstrom, H. (2006). Effects of three different swallow maneuvers analyzed by videomanometry [Electronic version]. Acta Radiologica, 47, 628-633. Retrieved 2/1/09, from EBSCOhost database.
This study was conducted to analyze how different swallowing maneuvers such as the super-supraglottic, supraglottic, and Mendelsohn affect swallowing in healthy volunteers. Videoradiography and manometry were used to analyze the upper esophageal constriction during the pharyngeal phase of three types of swallowing maneuvers. Pharyngeal manometry is the recording of muscle pressures used for the quantitative evaluation of the upper esophageal sphincter (UES).
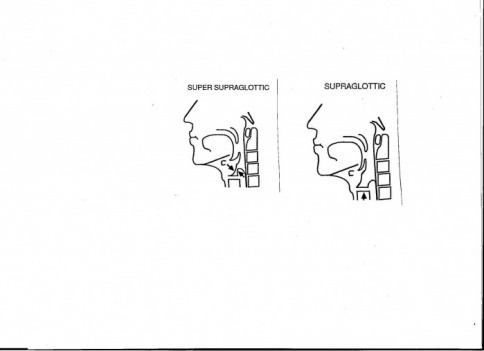
The supraglottic swallow is designed to close the true vocal cords before and during swallowing to prevent the entry of food into the airways. This technique involves breathholding before and during the pharyngeal phase of swallowing. The super-supraglottic swallow is designed to close the airway entrance above the true vocal cords and requires breathholding while bearing down which pulls the arytenoid cartilage forward to the base of the epiglottis and closes the laryngeal entrance at the level of the false vocal folds. Mendelsohn’s maneuver is designed to extend and prolong laryngeal elevation and thereby to prolong the UES opening during swallowing. This maneuver is further investigated through the relevant link. These are popular methods of improving swallowing in patients with dysphagia related to the oral and pharyngeal phases of swallowing.
The manometry catheter was positioned in the UES and the three transducers were each positioned at the level of the inferior pharyngeal constrictor muscle (PhiCi), the level of the superior pharyngeal constrictor muscle, and the base of the tongue. The seven variables analyzed during the manometric procedure were: pharyngeal peak contraction, pharyngeal peak duration, pharyngeal contraction rate, UES relaxation pressure, UES relaxation duration, coordination of the PhiCi-UES, and UES peak contraction. Video analysis was performed in slow motion frame by frame of bolus transit time and maximal hyoid movement.
Results show that the PhiCi peak pressure was significantly increased with the Mendelsohn maneuver and duration of the PhiCi contraction was significantly longer. The duration is individual and is due to how long the instructor has directed the volunteers to hold the larynx elevated. The effect of the increased contraction pressure in the pharynx may be that the propulsion of the bolus into the esophagus is improved as long as the airway is properly closed. The PhiCi contraction rate did not show any significant difference between the three swallow maneuvers and the control. The relaxation pressure of the UES was significantly increased in the super-supraglottic swallow compared to the control swallow. This might be due to the effort that is combined with breathholding, which might result in increased pressure. The UES relaxation duration was slightly shorter in the super-supraglottic swallow. The supraglottic and Mendelsohn maneuvers did not show any significant difference in UES relaxation pressure and duration. Coordination of the PhiCi contraction and the UES relaxation did not show any significant difference in the swallowing maneuvers, but the supraglottic swallow had a slightly earlier onset of the UES relaxation. The peak value of the UES contraction was significantly lower in all the swallows when compared to the control swallow. The bolus transit time was significantly prolonged in the super-supraglottic swallow and in the Mendelsohn maneuver compared to the control swallow this may be due to the increased UES relaxation pressure. The maximal hyoid movement did not show any significant differences in any of the maneuvers.
Both the supraglottic and the super-supraglottic maneuvers are designed to improve airway closure. It is hypothesized that because the supraglottic maneuver just includes breatholding during swallowing, it is unlikely that this maneuver will affect manometric values. The super-supraglottic maneuver has another technique with breathholding while bearing down. This might produce increased pressure in the PhiCi and the UES. The individuals performed the supraglottic swallow with great variance indicating that this technique either requires extensive training or that this technique works differently depending on how different individuals performed it.
Clinical experiences and data collection indicate these swallows are beneficial for improving nutritional intake and hydration. This study further describes the techniques and physiology of the mechanism during the pharyngeal phase of the swallow. There is a need for further research studies on swallowing techniques and their effects on the pharyngeal swallow in impaired individuals and healthy elderly volunteers.
